Friday 30 November 2012
MOTOR NEURON, ALS, LYME DISEASE
Despite that future research is still needed, some data of the literature suggest a possible relationship between ALS and Lyme disease.
References with respect to ALS and Borrelia burgdorferi
Lancet. 1987 Aug 8;2
(8554):332-3.
Borrelia burgdorferi antibodies and amyotrophic lateral sclerosis.
Waisbren BA, Cashman N, Schell RF,
Johnson R.
Muscle Nerve. 2009 Oct;40(4):626-8.
Lyme disease serology in amyotrophic lateral sclerosis.
Qureshi M,
Bedlack RS, Cudkowicz ME.
Source
Neurology Clinical Trials Unit, Massachusetts General Hospital, Harvard Medical
School, 13th Street, Building 149, Room 2274, Charlestown, Massachusetts 02129, USA.mqureshi@partners.org
Abstract
Lyme disease is sometimes part of the differential diagnosis for amyotrophic lateral sclerosis (ALS). Herein we report on 414 individuals with ALS at the Massachusetts General Hospital who underwent laboratory testing for Lyme disease.
Twenty-four (5.8%) were seropositive, but only 4 (0.97%) had confirmed past immunoreactive infection. Two of these patients received ceftriaxone for 1 month without clinical improvement. Lyme disease was rare in 414 patients with ALS and is not likely to be causative.
Wien Med Wochenschr. 1995;145(7-8):186-8.
[ALS-like sequelae in chronic
neuroborreliosis].
[Article in German]
Hänsel Y, Ackerl M, Stanek G.
Source
Neurologischen Abteilung des Kaiser-Franz-
Josef-Spitals, Wien.
Abstract
CSF investigation in a 61-year old female patient with clinical picture of motoneuron
disease gave evidence for chronic infection with Borrelia burgdorferi. Improvement of clinical and CSF findings could be observed after antibiotic therapy. The diagnosis of amyotrophic lateral sclerosis which was initially suspected had to be revised and the disorder was interpreted as chronic neuroborreliosis.
Rev Neurol (Paris). 2006 Jun;162 Spec No 2:
4S50-4S56.
[What is the role of other complementary examination in amyotrophic lateral sclerosis?].
[Article in French]
Tranchant C.
Source
Département de Neurologie, Hôpitaux Universitaires, Strasbourg. Christine.Tranchant@chru-strasbourg.
fr
Abstract
Amotrophic lateral sclerosis diagnosis is based on clinical and electrophysiological findings. Transcranial
magnetic stimulation and MRI can show abnormalities which are not specific, but which can confirm upper motor neuron involvement. The other tests are performed to exclude differential diagnosis. Tests which should be performed in every cases are: medullar MRI, blood counts, erythrocyte sedimentation, serum protein electrophoresis, calcium, phosphore,
serological tests for HIV, siphylis, Lyme disease. Other tests are made in some clinical circonstances to exclude genetical disease or metabolic disorders (SMN gene, Kennedy gene, Hexosaminidase A, very long chaine fatty acids), haematological or paraneoplasic disorders (anti-neurons antibodies, PSA, CT of chest and abdomen, mammography, bone
marrow biopsy) or inclusion myositis (muscle biopsy).
Wien Med Wochenschr. 1995;145(7-8):186-8.
[ALS-like sequelae in
chronic neuroborreliosis].
[Article in German]
Hänsel Y, Ackerl M, Stanek G.
Source
Neurologischen Abteilung des Kaiser-
Franz-Josef-Spitals, Wien.
Abstract
CSF investigation in a 61-year old female patient with clinical picture of motoneuron disease gave evidence for chronic infection with Borrelia burgdorferi. Improvement of clinical and CSF findings could be observed after antibiotic therapy. The diagnosis of amyotrophic lateral sclerosis which was initially suspected had to be revised and the disorder was interpreted as chronic neuroborreliosis.
PMID: 7610670 [PubMed -
indexed for MEDLINE]
Arch Neurol. 1990 May;47(5):586-94.
Immunologic reactivity against Borrelia burgdorferi in
patients with motor neuron disease.
Halperin JJ, Kaplan GP, Brazinsky S, Tsai TF, Cheng T, Ironside A, Wu P, Delfiner
J, Golightly M, Brown RH, et al.
Source
Department of Neurology, State University of New York, Stony Brook 11794.
Abstract
Of 19 unselected patients with the diagnosis of amyotrophic lateral sclerosis (ALS) living in Suffolk County, New York (an area of high Lyme disease prevalence), 9 had serologic evidence of exposure to Borrelia burgdorferi; 4 of 38 matched controls were seropositive. Eight of 9 seropositive patients were male (8 of 12 male patients vs 2 of 24 controls). Rates of seropositivity were lower among patients with ALS from nonendemic areas. All patients had typical ALS; none had typical Lyme disease. Cerebrospinal fluid was examined in 24 ALS patients--3 (all with severe bulbar involvement) appeared to have intrathecal synthesis of anti-B burgdorferi antibody. Following therapy with antibiotics, 3 patients with predominantly lower motor neuron abnormalities appeared to improve, 3 with severe bulbar dysfunction deteriorated rapidly, and all others appeared unaffected. There appears to be a statistically significant association between ALS and immunoreactivity to B burgdorferi, at least among men living in hyperendemic areas.
Wednesday 28 November 2012
LYME DISEASE TREATMENT NHS
Lyme Disease treatment on the NHS has been a very controversial area for those patients who fail the usual couple of weeks antibiotics usually given by NHS doctors following the HPA guidance. That is when they are treated in the early stages of the illness, because so many of us missed that window of opportunity despite seeking medical attention for tick bites, bulls eye rashes, summer flu' and migrating arthralgias.
Lyme Disease Action charity has been working with the James Lind Alliance reviewing the available research on diagnosis and treatment of Lyme disease looking for areas of uncertainties.
The James Lind Alliance is funded by the National Institute for Health.
Links to the Lyme disease Action website here
Links to more than 39 uncertainties here
Doctors and patients or their carers can vote on the top ten priorities for research before the 9th December 2012 here
Hopefully this research will be brought to the attention of doctors who frequently fail to even recognise the certainties of Lyme Disease such as the EM Rash -
'Does EM provide an ‘accurate’ clinical diagnosis of LD?
Yes it does. See Stanek G, Fingerle V, Hunfeld K, Jaulhac B, Kaiser R, Krause A, et al. Lyme
borreliosis: clinical case definitions for diagnosis and management in Europe. Clinical
Microbiology and Infection. 2011 Jan;17(1):69–79.
In correspondence from the Dept of Health, Earl Howe, 12.12.2011 via my MP Anne Milton .The Dept of Health says 'The Department is working with Lyme Disease Action (LDA) and I am aware that you as Health minister, have met with LDA representatives. We are supporting its initiative with the James Lind Alliance and await the findings of their review.'
I look forward to more information about these uncertainties being relayed to our treating doctors and consultants and changes to existing guidance from the Dept of Health via the Health Protection Agency reflecting that there are many uncertainties, instead of the current restrictive guidance based more on opinion than scientific data.
By identifying uncertainties in the research hopefully in time research will be directed into these areas that need more detailed investigation.
Lyme Disease Action charity has been working with the James Lind Alliance reviewing the available research on diagnosis and treatment of Lyme disease looking for areas of uncertainties.
The James Lind Alliance is funded by the National Institute for Health.
Links to the Lyme disease Action website here
Links to more than 39 uncertainties here
Doctors and patients or their carers can vote on the top ten priorities for research before the 9th December 2012 here
Hopefully this research will be brought to the attention of doctors who frequently fail to even recognise the certainties of Lyme Disease such as the EM Rash -
'Does EM provide an ‘accurate’ clinical diagnosis of LD?
Yes it does. See Stanek G, Fingerle V, Hunfeld K, Jaulhac B, Kaiser R, Krause A, et al. Lyme
borreliosis: clinical case definitions for diagnosis and management in Europe. Clinical
Microbiology and Infection. 2011 Jan;17(1):69–79.
In correspondence from the Dept of Health, Earl Howe, 12.12.2011 via my MP Anne Milton .The Dept of Health says 'The Department is working with Lyme Disease Action (LDA) and I am aware that you as Health minister, have met with LDA representatives. We are supporting its initiative with the James Lind Alliance and await the findings of their review.'
I look forward to more information about these uncertainties being relayed to our treating doctors and consultants and changes to existing guidance from the Dept of Health via the Health Protection Agency reflecting that there are many uncertainties, instead of the current restrictive guidance based more on opinion than scientific data.
By identifying uncertainties in the research hopefully in time research will be directed into these areas that need more detailed investigation.
Saturday 24 November 2012
MOTOR NEURON DISEASE/ALS STABILIZED ON LONG TERM ANTIBIOTICS
Sharing from a friend with a link to a post on my blog about him here
The translation is thanks to Google so apologise for errors but you get the idea.
Dear Joanne
would you please translate this to English? Its a column to have been underwritten wooden i will send to ILADS guys! borreliasyk I've been in 12 years.
Like many others, I have not been believed that the Norwegian health care system that diagnosed me with ALS. I've driven trial twice. Lost both. This despite the fact that I tested positive on the Western Blot test, tested positive at the Vestfold Hospital and found Borrelia DNA in my blood in 2009.
I sometimes have a feeling of being involuntary participant in an academic parlor game. It's as if most of the health care system sees this as a game - and not as a prolonged, intense and bitter struggle for life and health. , we have a large group of seriously ill patients who have good reason to believe that a Borrelia infection is the underlying cause - but are banned from using the device with a negative antibody test (often Elisa) as justification.
In 12 years I have accumulated knowledge about the disease, but it seems that doctors have a monopoly on qualified opinions. Because of their status, they can decide what is the scope for credible evidence to justify saying their opinions.
If they encounter documentation that goes across their opinions, they may with ease doubt about it. Or so they know not to studies and publications that make their arguments fall through. The latter is probably hard to recognize, so it will be easier to call documentation implausible.
I refer to the magazine's story about how Borrelia among others Dr. Jon Sundal attended. He was also an expert witness against me in the trial. I'm not looking for the actual content of the program, but there are general attitudes Sundal have, I want to life!
One tries to persuade public opinion that good western blot tests often give false positive responses, which is incorrect tests based on several numerical markers that identify Borrelia bacterium. Some markers are nonspecific and may cross react with other bacteria, while some markers are specific borrelia "fingerprint" - markers. Mon. require a certain number of markers to be regarded as positive for declaring the test as positive.
This will make it easier to evaluate the tests. requirement to have a positive test, three of these specific markers.
The American Health Authority (CDC) has recognized my test as secure positive. micrograms recombinant western blot (immunoblot) containing antigen that captures all strains of Borrelia bacteria. It does not Elisa! . Recommended Vestfold Hospital (SIV's) MIKROGEN recombinant western blot that is the best test.
The problem is again money. The test is expensive and time consuming. This must be funded! SIV has expertise and a highly skilled specialists!
Sundal also claims that one must have inflammatory cells in the spinal fluid of having neuroborreliosis. This Slovenian researcher Franck Strle proven wrong. He is with Hunfeld Fingerle Wilske and Stanek among tungtvektekterne in Europa.Også laboratories in Norway have discovered this! Unfortunately, doctors are not updated for this No, absolutely no Norwegian attending their seminars! Only a retired doctor, Per Bjarke.
False negative tests dominate. Therefore, it is dangerous to allude that Elisa tests are good enough. Lori Bakken conducted a double-blind study showed that not only was Elisa inaccuracies between competing laboratories, but the same laboratory showed different results on the same sample. Only 45 laboratories had a score of 55 percent.
Another study was conducted by the College of American Patholigists. The result was terrible. It was similar to the same number of false positives as false negatives. Only 45 percent of the 516 laboratories that tested showed the correct answer. It entered that stage I of the disease discovers Elisa 20-50 percent of cases and in stage II / III 70-100 percent, depending on the tests used.
Some argue that sensitivity in stage II / III is not more than 20-80 per cent. The tests used in the cerebrospinal fluid in Norway today finds no more than 50 percent: 70 percent for garinii and 10 percent for afzelii, which is the most common borrelia strain circulating in Norway due to false negative results are numerous.
The bacteria manipulate our immune system so that we do not produce antibodies. Antibodies are very late in forføpet. The bacteria can lie in niches inside the cells of the organs where it is hidden from the immune system. The bacterium converted to cyst forms with new antigens that are not found in the tests available today.
The tests used today are quite specific as false positive is not a big problem. False negatives, however, problematic. This is why clinic and patients' own history is so important in the overall assessment. I think Western blot should be emphasized rather than as indirect Elisa test. The sensitivity has been discussed regarding western blot, but specific band in the test should be a clear indicator of Borrelia infection.
ANTIBIOTICS For chronically ill have a pulsating regime (periodic time) high doses of ceftriaxone IV has been a success. This was published in the early 90's and was confirmed on MLDA Lyme congress in 2002. treatment should be individualized on both the dosage and length.
Stricker refers to studies where long-term antibiotic treatment is far better than the standard treatment. Klempners standard (Dr Mark Klem opens conducted a study on the treatment of patients. Though the study had clear deficiencies, it has been accepted as standard. Probably why we have several cases of illness due under treatment) in a month ceftriaxone IV and two months of oral doxycycklin, had little effect on chronic borrelia or come late disease.
Increased improvement the longer treatment duration was noticeable. This is published in the CID that is a IDSA (Infectious Disease Society of America). Looks like IDSA turns when they choose to publish this. So in these cases must be treated for months and even years with antibiotics.
Change of combination treatments may be necessary. Must be individualized. It is vital to acknowledge this since late come and chronic Borrelia ill probably have chronic infection combined with additional infections. Therefore, required prolonged treatment. Therefore I genuinely sorry when doctors refuse patients treatment! There is no reason to doubt that prolonged treatment helps some.
According to statistics I should have been dead 10 years ago! I'm probably the only one in the world who has lived with ALS diagnosis in 12 years, which can stand on their feet and do not need a respirator! Court, the appeal board patient and their experts find it more probable than that I have borrelia.
Fortunately rescued antibiotics I received in the USA for 03 my life! I had to go. Here at home did not help! Health care is often concerned with the ethical dimension. As I see it, it is the exclusion of Lyme disease patients is the greatest ethical challenge. These patients (assuming they indisputably have very severe disease) are invited ME diagnosis or ALS without other evidence than that it can not be anything else.
It may NOT be ethically problematic to make treatment studies in this group of patients. They get anyway no qualified help. I will fight for us, as long as there is life in me.
Eivind Markhus
Friday 23 November 2012
TREATMENT TO REVERSE MOTOR NEURON DISEASE.
'Any therapy which is capable of reversing the untreated
natural history of Motor Neuron Disease is Press-worthy.'
inmacdonald- Posts: 548
- Joined: Fri 13 Jan 2012 22:32

Wednesday 21 November 2012
WHAT CAUSES WHITE MATTER LESIONS IN THE BRAIN OF PATIENTS WITH MULTIPLE SCLEROSIS - HOW SOME CAN BE IMPROVED.
Early signs of Multiple Sclerosis were thought to be lesions in the white matter of the brain, new research discusses disease progression and finds that it is a process starting outside of the brain.
Multiple sclerosis (MS) may progress from the outermost layers of the brain to its deep parts, and isn’t always an “inside-out” process as previously thought, reported a new collaborative study from researchers at the Mayo Clinic and the Cleveland Clinic. The traditional understanding is that the disease begins in the white matter that forms the bulk of the brain’s inside, and extends to involve the brain’s superficial layers, the cortex. Study findings support an opposite, outside-in process: from the cerebrospinal fluid-filled subarachnoid space, that cushions the outside of the brain and the cortex, into the white matter. The new findings will guide researchers as they seek to further understand and treat the disease. The study was published in the December 8th, 20011 issue of the New England Journal of Medicine.
Link to these research findings here
It says 'the early lesions were highly inflammatory'
It has been recognised for some time that some MS cases can be caused by infections such as Chamydia Pneumonia websites here and here
and Lyme Disease.
Microbiologist Thomas Grier has lectured extensively on Lyme disease and Multiple Sclerosis, links to several of his lectures are posted in the right hand column of this blog.
Below was Tom's response to the new MS research :-
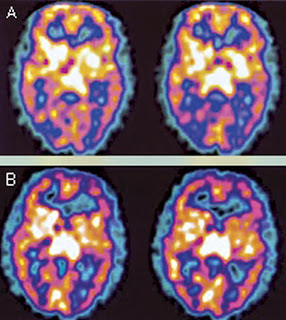
Figure 2
Multiple sclerosis (MS) may progress from the outermost layers of the brain to its deep parts, and isn’t always an “inside-out” process as previously thought, reported a new collaborative study from researchers at the Mayo Clinic and the Cleveland Clinic. The traditional understanding is that the disease begins in the white matter that forms the bulk of the brain’s inside, and extends to involve the brain’s superficial layers, the cortex. Study findings support an opposite, outside-in process: from the cerebrospinal fluid-filled subarachnoid space, that cushions the outside of the brain and the cortex, into the white matter. The new findings will guide researchers as they seek to further understand and treat the disease. The study was published in the December 8th, 20011 issue of the New England Journal of Medicine.
Link to these research findings here
It says 'the early lesions were highly inflammatory'
It has been recognised for some time that some MS cases can be caused by infections such as Chamydia Pneumonia websites here and here
and Lyme Disease.
Microbiologist Thomas Grier has lectured extensively on Lyme disease and Multiple Sclerosis, links to several of his lectures are posted in the right hand column of this blog.
Below was Tom's response to the new MS research :-
The observation that early MS begins with inflammation in the outer cortical regions of the brain seems to fit with the physiology of the location of the BBB and the close proximity to microglia cells, an arrangement that suggests something is crossing the BBB to initiate inflammation and vessel infiltrate.
It is also interesting that white matter lesions later on seem to aggregate around or near the central ventricles often with micro-vessel inflammation/infiltrate seen in the ependyma membrane of the ventricles. This also suggests some outside factor is entering from the “Outside-In” through the CSF.
The spirochete hypothesis of sclerosing pathology suggested by myself, suggests that Borrelia (various species) enter through the BBB and inflame the vessels and activate microglia. Some motile bacteria may also enter the subarachnoid space a place spirochetes cannot thrive and then find their way to the ventricles-ependyma and back into blood vessels where spirochetes can find a more favorable environment. Increases in quinolinic acid levels from BBB-junction inflammation may also contribute to white matter destruction without the direct presence of the bacteria in the white matter lesions. (Spirochetes are more often found in the gray-matter)
This is born out by the lack of spirochetes found in white matter lesions, but classical forms when found, are almost always in the gray matter. This can be seen by using silver stains combined with microwave deflation of the fresh brain cells allowing the spirochetes from many levels becoming visible as the metal coated bacteria rise through the collapsed brain tissue.
This spirochete sclerosing model addresses
1) cortical gray-matter inflammation,
2) rise of an inflammatory toxin of demyelination Quinolinic Acid
3) a mechanism that explains periventricular inflammation and lesions secondary to BBB breakdown and gray-matter inflammation.
4) A possible reason for heterogeneous plagues prevailing
5) The increased incidence of MS in Lyme endemic areas
6) Intracellular infection in neurons explains lack of positive serology tests and patient relapses after antibiotics.
1) cortical gray-matter inflammation,
2) rise of an inflammatory toxin of demyelination Quinolinic Acid
3) a mechanism that explains periventricular inflammation and lesions secondary to BBB breakdown and gray-matter inflammation.
4) A possible reason for heterogeneous plagues prevailing
5) The increased incidence of MS in Lyme endemic areas
6) Intracellular infection in neurons explains lack of positive serology tests and patient relapses after antibiotics.
It seems that if spirochetes play a role in forming some plaques similar to MS plaques, then in order to get good data for treatment research we must consider trying to separate the Spirochete Sclerosing componant from the rest of the data.
For example an immune modulating drug might help true MS but if the data is mixed with patients from Lyme endemic areas that have not been separated in these trials, then treatment may have brief improvement and then a worsening without knowing which patients have an infectious component.
In the hundreds of biopsies used in this study were any also stained with anti-Borrelia antibody fluorescent stains or silver stains? If not we can make no conclusions that spirochetes did not play a role in the gray-matter pathologies.
Tom Grier (A survivor a primary progressive MS)
Earlier this year research by Sam Donta here
SPECT Brain Imaging in Chronic Lyme Disease
Conclusions: Brain SPECT scans are abnormal in most patients with chronic Lyme disease, and these scans can be used to provide objective evidence in support of the clinical diagnosis. The use of certain antibiotic regimens seems to provide improvement in both clinical status and SPECT scans.

Figure 2
FIGURE 2. SPECT scan of the brain before (A) and after (B) antibiotic treatment. These transaxial images are from a 51-year-old man diagnosed with Lyme disease with a recent change in memory. Representative pretreatment images show hypoperfusion within the mid posterior and mid temporoparietal cortex bilaterally. Representative posttreatment images (14 months later) reveal improved perfusion to the posterior temporoparietal cortex bilaterally, correlating with improved symptoms. Perfusion within the remaining cerebral cortex, basal ganglia, thalamus, and cerebellum was normal.
Sunday 18 November 2012
WHY DO MY SYMPTOMS IMPROVE ON ANTIBIOTICS BUT DETERIORATE WHEN I STOP?
Why does my arthritis get better when I take antibiotics but deteriorate when I stop?
Why does my muscle weakness get better on antibiotics but deteriorate when I stop?
Why does my fatigue and Fibromyalgia get better when I take antibiotics but deteriorate when I stop?
Why do my chronic symptoms improve on antibiotics for urinary tract infection and then deteriorate when antibiotics stop?
Why do my neurological symptoms get better on antibiotics and deteriorate when I stop?
I hear these questions all the time from people with RA, ME/CFS, Fibromyalgia, MS, Parkinson's - read any Facebook site for these illnesses and you see it over and over.
Well in my case it turned out that I had Lyme Disease but no doubt there are other bacterial infections that are not cleared by just a couple of courses of antibiotics.
Biofilms is one reason why Borrelia ( Lyme Disease) can persist despite long term antibiotics.

Dr MacDonald pathologist and researcher of Lyme Borreliosis gives us a good lesson on Biofilms of Borrelia- from Lymenet Europe here
We now have entered a third era in Lyme Borreliosis - namely the Biofilm Era.
Biofilms of borrelia burgdorferi were undreamed of until year 2006 and proven to exist in vitro and recently In ViVO in human skin biopsies of Erythema Migrans and in living Ixodid Tick midguts.
Biofilm science is radically different from Planktonic microbiology. Biofilms are part of the
repertoire of over 99.9% of microbes. Biofilms form from planktonic microbial forms, but
biofilms provide mechanisms for microbial survival under adverse conditions which would eliminate
planktonic microbes. Biofilms explain Chronic antibiotic resistance. Biofilms are the mechanism
for Chronic Infections of many organ systems. The diagnostic names - infected artificial medical
device, bacterial endocarditis, Helicobacter pylori chronic gastritis, Dental root canal infections,
and may more- have the concept that these infections are solely due to biofilmsand the persistence of
biofilms in humans despite administration of antibiotics/
In biofilms the microbes {planktonic forms} undergo specialization and are no longer
identical to Planktonic [single free living microbes]. Biofilm microbes are biochemically specializing
(ie have a different biochemistry, different cell wall structure, have cell to cell intercommunications
[nanowires and nanotubes] which enable cell to cell communication between the cytoplasmic compartments, and form water channels to facilitate the flux of nutrients and the removal of waste
from the biofilm community. An envelope of Extracellular matrix invests biofilm communites. This matrix is derived from once living --now dead members of the biofilm community. For Borrelia biofilms
the matrix investment includes Sloughed Outer Surface Membrane {slime layer} of Bb, Extruded
DNA [eDNA], alginate-like material, and liposomes {micro vesicles} [blebs].
Biofilm communities may be and often are POLYMICROBIAL.
Biofilm communities spread from their sessile site of naissance to the body sites by
two mechanisms:
1. pieces of the Sessile community [Matrix invested specialized microbes] actually break apart
from the parent community and METASTASIZE to other sites.
2. Planktonic Showers rain from the sessile community from time to time and these
planktonic showers re-establish new communities in the mammalian host.
So in the year 2102, we have now entered into the 3rd era of Borrelia pathobiology;
namely the Biofilm Era.
Implicit in the biofilm concept is the ability of DNA transfer/exchange
[lateral DNA Transfer/ horizontal DNA transfer] among specialized members of the biofilm.
With DNa exchange, there is a mechanism for transfer of new virulence factors and new
modalities in antibiotic resistance. Persistence of biofilm infection in mammalian hosts
is in part due to PERSISTER microbes, which may reside within biofilm communities or which may reside intracellularly, or which may reside in so called "Sanctuary Sites"
The clinical spectrum of Lyme borreliosis continues to expand into areas of medicine
in which NAMED diseases of unknown cause [idiopathic diseases] are now incorporated within
the Lyme borreliosis disease complex. The number of skin conditions which are now Lyme disease
cutaneous manifestations has increased, thanks to the work of Dr Klaus Eisendle and Dr Bernhard Zelger to include many new entities, [ and more to be added with the use of FFM techniques]
I summarize these in my lecture on the International Cutaneous and Molecular Dermatopathology
of Lyme Borreliosis [attached , Boston Mass , Date November 4,2012]
In parallel with the expansion of cutaneous Borreliosis conditions, is the expansion of lymphoid
neoplasias linked to chronic Borrelia infections [ analogy with Helicobacter pylori induced
Malignant Lymphomas], Sarcoidosis in China as a borreliosis infection, Idiopathic lethal fibrosing
illnesses [Retroperitoneal Fibrosis, and Mediastinal fibrosis], borrelia to human Tranfections
mimicking human spontaneous gene mutations, Cardiomyopathies secondary to chronic Lyme borreliosis, giant cell arteritis [temporal arteritis] due to borrelia infection, Abdominal aortic aneurysms due to borrelia aortitis, and various intra-ocular inflammations {uveitis, optic neuritis},
Demyelination syndromes secondary to borrelia infections, and transplacental transmission of borrelia with possible lethal outcomes in the fetus in untreated conditions. The list above is only partial and will be added
to as future medical research utilizing molecular Tools such as DNA probes fleshes out the full spectrum of
Lyme borreliosis and related co-infections.
It is truly a great time to be alive.
With all good wishes,
Alan
An earlier post on biofilms and Borrelia here
Dr Alan B MacDonald has already earned a Nobel Prize several times over in my view for the services he has done to the science and medicine in the field of Lyme Borreliosis I hope I am still around to see him recognised for those services.
Why does my muscle weakness get better on antibiotics but deteriorate when I stop?
Why does my fatigue and Fibromyalgia get better when I take antibiotics but deteriorate when I stop?
Why do my chronic symptoms improve on antibiotics for urinary tract infection and then deteriorate when antibiotics stop?
Why do my neurological symptoms get better on antibiotics and deteriorate when I stop?
I hear these questions all the time from people with RA, ME/CFS, Fibromyalgia, MS, Parkinson's - read any Facebook site for these illnesses and you see it over and over.
Well in my case it turned out that I had Lyme Disease but no doubt there are other bacterial infections that are not cleared by just a couple of courses of antibiotics.
Biofilms is one reason why Borrelia ( Lyme Disease) can persist despite long term antibiotics.

Dr MacDonald pathologist and researcher of Lyme Borreliosis gives us a good lesson on Biofilms of Borrelia- from Lymenet Europe here
We now have entered a third era in Lyme Borreliosis - namely the Biofilm Era.
Biofilms of borrelia burgdorferi were undreamed of until year 2006 and proven to exist in vitro and recently In ViVO in human skin biopsies of Erythema Migrans and in living Ixodid Tick midguts.
Biofilm science is radically different from Planktonic microbiology. Biofilms are part of the
repertoire of over 99.9% of microbes. Biofilms form from planktonic microbial forms, but
biofilms provide mechanisms for microbial survival under adverse conditions which would eliminate
planktonic microbes. Biofilms explain Chronic antibiotic resistance. Biofilms are the mechanism
for Chronic Infections of many organ systems. The diagnostic names - infected artificial medical
device, bacterial endocarditis, Helicobacter pylori chronic gastritis, Dental root canal infections,
and may more- have the concept that these infections are solely due to biofilmsand the persistence of
biofilms in humans despite administration of antibiotics/
In biofilms the microbes {planktonic forms} undergo specialization and are no longer
identical to Planktonic [single free living microbes]. Biofilm microbes are biochemically specializing
(ie have a different biochemistry, different cell wall structure, have cell to cell intercommunications
[nanowires and nanotubes] which enable cell to cell communication between the cytoplasmic compartments, and form water channels to facilitate the flux of nutrients and the removal of waste
from the biofilm community. An envelope of Extracellular matrix invests biofilm communites. This matrix is derived from once living --now dead members of the biofilm community. For Borrelia biofilms
the matrix investment includes Sloughed Outer Surface Membrane {slime layer} of Bb, Extruded
DNA [eDNA], alginate-like material, and liposomes {micro vesicles} [blebs].
Biofilm communities may be and often are POLYMICROBIAL.
Biofilm communities spread from their sessile site of naissance to the body sites by
two mechanisms:
1. pieces of the Sessile community [Matrix invested specialized microbes] actually break apart
from the parent community and METASTASIZE to other sites.
2. Planktonic Showers rain from the sessile community from time to time and these
planktonic showers re-establish new communities in the mammalian host.
So in the year 2102, we have now entered into the 3rd era of Borrelia pathobiology;
namely the Biofilm Era.
Implicit in the biofilm concept is the ability of DNA transfer/exchange
[lateral DNA Transfer/ horizontal DNA transfer] among specialized members of the biofilm.
With DNa exchange, there is a mechanism for transfer of new virulence factors and new
modalities in antibiotic resistance. Persistence of biofilm infection in mammalian hosts
is in part due to PERSISTER microbes, which may reside within biofilm communities or which may reside intracellularly, or which may reside in so called "Sanctuary Sites"
The clinical spectrum of Lyme borreliosis continues to expand into areas of medicine
in which NAMED diseases of unknown cause [idiopathic diseases] are now incorporated within
the Lyme borreliosis disease complex. The number of skin conditions which are now Lyme disease
cutaneous manifestations has increased, thanks to the work of Dr Klaus Eisendle and Dr Bernhard Zelger to include many new entities, [ and more to be added with the use of FFM techniques]
I summarize these in my lecture on the International Cutaneous and Molecular Dermatopathology
of Lyme Borreliosis [attached , Boston Mass , Date November 4,2012]
In parallel with the expansion of cutaneous Borreliosis conditions, is the expansion of lymphoid
neoplasias linked to chronic Borrelia infections [ analogy with Helicobacter pylori induced
Malignant Lymphomas], Sarcoidosis in China as a borreliosis infection, Idiopathic lethal fibrosing
illnesses [Retroperitoneal Fibrosis, and Mediastinal fibrosis], borrelia to human Tranfections
mimicking human spontaneous gene mutations, Cardiomyopathies secondary to chronic Lyme borreliosis, giant cell arteritis [temporal arteritis] due to borrelia infection, Abdominal aortic aneurysms due to borrelia aortitis, and various intra-ocular inflammations {uveitis, optic neuritis},
Demyelination syndromes secondary to borrelia infections, and transplacental transmission of borrelia with possible lethal outcomes in the fetus in untreated conditions. The list above is only partial and will be added
to as future medical research utilizing molecular Tools such as DNA probes fleshes out the full spectrum of
Lyme borreliosis and related co-infections.
It is truly a great time to be alive.
With all good wishes,
Alan
An earlier post on biofilms and Borrelia here
Dr Alan B MacDonald has already earned a Nobel Prize several times over in my view for the services he has done to the science and medicine in the field of Lyme Borreliosis I hope I am still around to see him recognised for those services.
Saturday 10 November 2012
LYME DISEASE SYMPTOMS - COMPREHENSIVE LIST.
Most doctors are unaware of the many ways that Lyme Disease can affect patients so I am copying and posting this open letter that Dr Alan B MacDonald sent to Carter Blakely on Wellness Guidelines which includes a comprehensive list of conditions that can be related to an infection of Lyme Disease. Thanks to Dr MacDonald for posting on Lymenet Europe link here
Subscribe to:
Posts (Atom)